Veterinarian, PhD, Expert in Equine Laminitis and other pathologies of the horse's foot
What is the Corium?
Corium is the skin that produces the hoofcapsule. It is the most delicate, vascularized and innervated structure of the strong horse’s body and since it is closed inside a very hard horn hoofcapsule it goes unnoticed to those who do not completely dedicate themselves to the foot. We all know “NO FOOT NO HORSE” as denial, but very few like myself, has dedicated the life to the positive improvement and protection of the germinative layer of the Hoof, the Corium to reverse in “BETTER CORIUM BETTER HORSE”. A mission dedicated to solving the paradox of the work of veterinarians and farriers who work on robust bodies and hooves with direct consequences on this tissue extremely vulnerable and invisible to the non-expert and specialized eye
In my professional activity as doctor and teacher I have understood over time that the Corium is the problem and at the same time the solution of the so much nebulous and discussed “Laminits”. As a matter of fact, the skin that produces the horn of the hoof called nail is easily visible to the human since the nail is transparent; while in the horse the hoof is thick and pigmented and therefore the Corium is not seen “unaided eye”. Only with ablative surgery “alive” or “dead” and with a radiographic contrast liquid, i.e. venography you can see the Corium. I was interested and dedicated not only to standardize this imaging technique, but also to develop it in order to see the immediate and long-term variations of the blood flow to the Corium, which depend maynly on biomechanical venous compression or other factors influencing the structure of the dermo-epidermal gear like lytic enzymes or toxic factor or bacteria.
How do you see the Corium? Venography
You can clearly see it is not easy to observe the Corium in these anatomical dissections, impossible in normal radiography.
In anatomical dissections in “dead horses” you loose the biomechanical influences of the weight of the horse on the Corium vascular bed (venuncompression). So, I observed that it is easier to obtain an arteriography with the horse in lateral decubitus, and easier to obtain a venography with the horse standing.




The best diagnostic tool to see Corium in the alive horse’s foot is Venography
Troncular anesthesia of the medial and lateral palmar nerves is performed, at the level of the apex of the sesamoids, with 2% Lidocaine to desensitize the finger, 10 ml subcutaneously is used for each injection site. The horse is then sedated with detomidine, the hooves are carefully cleaned of any residue and positioned on the appropriate podoblocks. At this point the adhesive bandage is placed around the fetlock, on which the tourniquet will be fixed, which acts as a tourniquet. This must be fixed tightly, in order not to incur trivial diagnostic errors related to the “leak” of liquid as for example by placing the tourniquet in the middle of the cannon as described for local antibiotic perfusion.
Once the tourniquet is fixed, the skin in correspondence with the lateral or medial palmar digital vein is disinfected with alcohol, the vein is catheterized with a 21G butterfly needle and the blood is allowed to flow until the tube is completely filled, then it is closed with the cap with perforable membrane.
At this point the tube is fixed to the same tensoplast used to stop the tourniquet and 20-25-30cc of contrast fluid are injected, being extremely careful not to break the vein, using very light pressure for this purpose. If the vein gives way, the lateral counter can be used. Once all the fluid has been injected, the first four radiographs are taken in 30-40 seconds, to obtain optimal images, before the contrast fluid can be partially absorbed by the tissues surrounding the blood vessels.
The images to be acquired are:






However, it is not at all easy to interpret the images by correlating them to the level of severity and risk and this diagnostic action must be referred to the expert dedicated solely to the horse’s foot.
The venogram is an indispensable clinical diagnostic tool for observing “in vivo” the finger’s vascular bed and the mechanical compression of the venous plexuses of the coronet and arterial plexuses of the sole in the standing horses, thanks to the use of contrast liquid, since the equine hoof is not as transparent as the human nail.
Regular monitoring using this imaging technique helps to better understand the sometimes cryptic history of the disease and allows for a targeted therapeutic strategy. In addition, the venogram has predictive potential, and allows the doctor to anticipate and treat soft tissue damages before they are detectable by X-ray exams without contrast.
How does the Corium change color?
the measurement of blood flow in the Corium is a singular importance in the horse’s finger which, being devoid of muscles, presents considerable problems of blood return to the heart and lymphatic plexuses. The exchange and increase in blood flow obviously brings more oxygen for the hemidesmosomes and desmosomes, in addition to the nutrients for the keratogenic and keratophore cells of the Corium. Consequently, the well vascularized Corium takes on a more bright red color, producing more horn and a better quality and density; on the other hand, the slightly oxygenated one tends to a blue-gray-black color and produces poor quality horny tissue to protect the Corium itself.
I personally developed and updated the Venogrphy technique in 2010 aming to observe the influence of weight of the horse in the 120 seconds available in the venographic examination in the 4 feet and 3 feet standing posture, in order to interpret the whites (radiopacity) and blacks (radiotransparence) of the radiography comparing them with several anatomical dissections in “ex vivo”. This allowed me to correlate the white color of our human finger with venous compression when we press on a surface.
I created an experiment that showed me what cannot be seen in the horse’s hoof standing by comparing the venographic images at a distance of a few seconds or minutes.



In twenty years of experience, I have been observing long-term changes of Venogram of the same horses for weeks, months and years. So, I could trained my mind and eyes to compare what is seen in human with what is not seen in the horse’s finger “in vivo” and I understand from the venographic images from the same horses, after a few days, weeks, months and years if the color of the Corium tends more to be pink-red or blue-gray-black in order to give a prognostic perspective of my patient in the short, medium and long term.

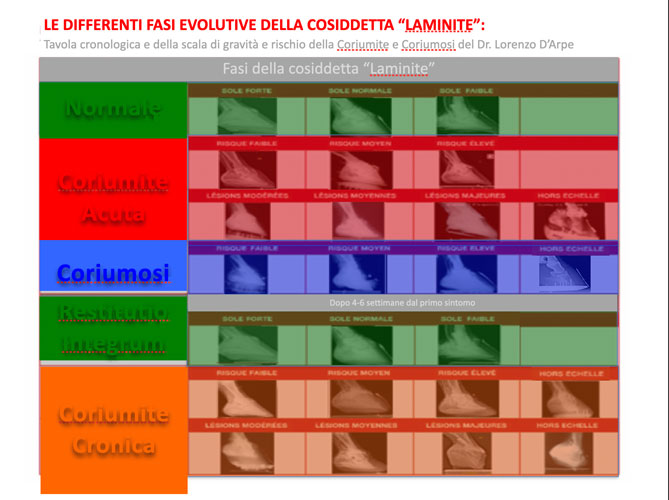
Collecting thousands of images in twenty years has allowed me to develop a flow chart inspired by Simon Curtis’ first try.
- in 1992 Using in vitro models, Pollitt CC was able to show retrograde filling of the digit’s arterial circulatory network when contrast fluid was injected in the digital vein.
- in 1993 Thereafter Redden RF used the Venogram as a diagnostic tool, in 2001 standardized a digital venography technique that can be used on standing horses.
- In 2007 A.Rucker described normal aspects of venogram
- In 2010 D’Arpe modified the technique
- In 2015 D’Arpe set the pathology flow chart and differentiated Coriumitis and Coriumosis
The Theory of 5 Hearts
2009
Theory of hydraulic pump of the Equine Foot.
Still today the most popular theory about the Equine foot dates back to the time of Aristotle and more recently documented by Delprier (1838), Bouley (1851), Bossi (1928) and Mensa (1965). The french authors wrote about the action of ungueal cartilage and the Italian authors discribe the similarity between the equine foot and the enclosed heart. In this old theory it was hypothesis that the load on frog and digital cushion induced the largement of the ungueal cartilages and consequently of the hoof capsule, called “elaterium” (elastic dilatation of the hoof). In 2009 I contradicted this old theory by exposing the formulation of the “5 Hearts” theory at the University of Lyon in France (oldest Vet school in the world). With respect for illustrious previous authors I tried to keep the heart-foot concept, but from the observations of the venograms on the Podoblock D’Arpe-Moreau which can flex-extend the horse’s finger in a tripodal station and after numerous anatomical dissections, I observed that the elaterium of the hoof and the opening and closing of the ungueal cartilages was due more to the flex- extension of the second phalanx rather than the fibrous digital cushion.
Later on I was able to do other experiments with considerably more advanced technologies on flexion of the finger extension “in vivo”. The study on Peripheral Venous Pressure between 2010 and 2013 and above all the measurement with EcoColor Doppler of the venous flow of the finger in 2014 made me deduce that in fact the foot acts only as a hydraulic shock absorber more than a pump. As a matter of fact also in the human the foot pump on the venous and lymphatic network is atribuited to the muscles of the leg abdomen, torax and heart more than the foot itself. The ungueal cartilages therefore act as safety valves ensuring the direction of the artero-venous flow and preventing arterial reflux during the loading phase. I then exposed this new theory in Lyon University in October 2014, contradicting my own previous theory. With deep respect for authors like Pollit who showed that only in the horse’s foot there is the same volume of blood as in the brain and furthermore in the standing posture without need even of walking the foot consumes as much energy as the equine brain; for all these reason I thought it was appropriate to call my new theory:”5 Brainstheory”.In this theory I attributed to the foot the function ofhydraulic shock absorber instead of hydraulic pump that is more likely due to the action of the muscles of the legs, abdomen, torax and heart.

The Theory of the 5 Brains
2014
How the horse world changes this new theory?
The “5 Brains new theory” means that to pump blood to the foot and improve its venous and lymphatic return it is not necessary to make horses with serious foot pathologies walk, but it is enough to induce small controlled contractions of the limb muscles by small balance instability. So you can avoid walking the horses with “Laminitis” out of the box because it worsens their condition by mechanically destroying the dermo-epidermal gear and it is much better to avoid putting the frog in contact with the ground because this way you only risks increasing trauma to Corium and the inflamation of the foot with sole bruises.From the observations of Redden and myself you can put self-massaging effects that create a slight instability under the CPS (Static Pressure Center, D. Levillard 2005) to induce muscles micro contraction controlled without lever arms under the foot. This muscles contractions improve blood pumping and veno-lymphatic emptying of the foot promoting and increasing blood circulation to the foot and to the whole finger and limb.
This hydraulic mechanism is dramaticaly important in the horse’s finger because there are no muscles and this is a major problem for blood return to the heart and lymphatic plexuses. The exchange and increase in blood flow obviously provides more oxygen for the hemidesmosomes and desmosomes and nutrients factors for the keratogen and keratophor cells of our beloved Corium tissue which will then have a nice color more tending to bright red rather than gray-black.
Thanks to Redden’s first clinical observations, I was in fact able to ascertain that the “self-massage effects” cause muscle microcontractions or fasciculations of the forearm and shoulder, without the need to make the horse move (move in space) in or out of the box.
I also observed with the experiments on the measurement of blood flow with PVP (Peripheral Venous Pressure) and Eco-Color Doppler that the micro muscle contractions favor the blood pumping and veno-lymphatic emptying of the foot, favoring and increasing the blood circulation of the foot and everything. the finger, limb, shoulder, thigh, abdomen and chest. In fact often horses with stasis edema of the hindquarters commonly called “swelling” or “engorgement” of the hindquarters using the self-massaging effects at night no longer need rest bands during the day.
100% of lame horses were healthy before, is your horse already lame or is it still healthy?
Have you ever thought about a disease prevention for your horse?
Come to find out, fill the form. I will be happy to meet you and prepare together the most suitable strategy for the health of your horse.


